Tampa, FL, January 24, 2020 – IDPodcasts’ state-of-the-art website platform has now entered its third decade of educating and informing an international audience with several all-new security enhancements. According to IDPodcasts editor-in-chief and webmaster, Dr. Richard Oehler, “The specific technology enhancements we’ve added may not be immediately recognized by many in our audience, but users will definitely recognize the performance improvements.”
The website has now migrated its hosting server to cPanel technology for improved reliability, hosting options, and backend website management. Meanwhile, security features have been significantly enhanced with the addition of an SSL certificate technology to improve data security between users and the website. Also, the website has incorporated robust firewall technology to reduce its vulnerability to hackers, malicious website intrusion, malware, ransomware, and other online threats.
“Users should notice usability improvements with the site and must know that we take their security and protection from online threats to be of the highest importance to us when they come to IDPodcasts.net,” Dr. Oehler states.
IDPodcasts was co-founded in 2007 by Dr. Richard L. Oehler, Professor of Medicine at the University of South Florida College of Medicine, and Dr. John T. Sinnott, current Chairman of the Department of Internal Medicine at the Morsani College of Medicine at USF. Dr. Oehler has been its editor-in chief and webmaster since its inception.
All of IDPodcast’s content is provided free to users, is self-sponsored, and is open access across the online universe. In addition to the YouTube Channel, IDPodcasts offers its content via smartphone and tablet apps, an iTunes Podcast series, and this website. New apps are currently under production for 2020 to bring an enhanced state-of-the-art IDPodcasts listening experience to the latest smartphone devices and tablets.
USF Infectious Diseases Fellows, From Left to Right: Dr. Vidhya Sabapathy, Dr. Ju Hee Katzman, Dr. Greg Teo, Dr. Carlos Lopez-Perez, and Dr. Andrew Nguyen
USF’s Infectious Diseases fellows and faculty were well-represented at the Infectious Diseases Society of America’s annual IDWeek ’19 session, held in Washington, D.C., from October 2 to 6, 2019. USF’s ID Division was collectively responsible for 14 poster presentations displayed between October 3rd through the 5th, and USF ID faculty Associate Professor Dr. Jamie Morano presented in a symposium on her experience in crafting the James A. Haley VA hospital’s outstanding ID Telehealth program, a national leader in the VA system.
A selection of the diverse poster sessions that were presented appears below:
Author and second-year ID fellow Ju Hee Katzman and her co-authors shared data on a series of 38 breast cancer patients who developed gram-negative skin and soft tissue infections following tissue expander surgery. The three most common pathogens found were Pseudomonas aeruginosa, Serratia marcescens, and Klebsiella pneumoniae. They concluded that in centers with a high percentage of gram-negative rods skin and soft tissue infections following tissue expander surgery, treating physicians should consider using perioperative antibiotics that include coverage against Pseudomonas, the most common isolate (45%).
Former (2017-2019) infectious disease fellow Dr. Shylah Moore and colleagues presented a poster on a five-year retrospective review within Florida’s Hillsborough County Department of Health comparing the trends and outcomes among HIV infected versus HIV uninfected patients with tuberculosis. Results suggested an HIV-TB coinfection rate that is slightly higher than the national population, with co-infected patients in the study sample having a statistically significant higher rate for cavitary TB.
Dr. Vidhya Sabapathy in front of her poster
Second year fellow Dr. Vidhya Sabapathy and colleagues reported on a retrospective analysis of 61 adult patients between 2010 and 2018 who were diagnosed and being treated for acute leukemia. All of the selected patients experienced severe neutropenia for 7 days or greater. Patient characteristics and infectious complications were examined. The most common diagnosis was AML. Bloodstream infections were the most common site, followed by respiratory tract infections. Gram-positive organisms were the leading etiology of bacteremias. In the subset of patients undergoing multiple induction chemotherapy, gram-negative pathogens were the leading cause of the bloodstream infections.
Dr. Shylah Moore and Colleagues’ Poster on Nocardia beijingensis
Dr. Shylah Moore, Dr. Johanna Asquith, and colleagues also reported on a retrospective chart review of 6 cases of a more recently described Nocardia strain first isolated in 2001 from sewage soil in China. The purpose of the study was to determine the risk factors and clinical manifestations of Nocardia beijingensis infection. All of the cases reviewed involved immunocompromised patients, were predominantly male, and had a mean age of 48. Most had lung involvement. Atypical manifestations included thecal sac infection and femur osteomyelitis. All isolates were susceptible to trimethoprim/sulfamethoxazole, but ceftriaxone and carbapenems were mostly used.
Dr. Carlos Perez-Lopez, a second year infectious diseases fellow and other co-authors reviewed a retrospective cohort of patients for seropositivity to Strongyloides stercoralis who underwent transplant evaluation from 2014-2016. A total of 228 charts were reviewed, and 113 seropositive patients were identified. Male gender and caucasian race predominated in both the seronegative and seropositive groups. The study did not find any statistically significant difference in the demographic characteristics or risk factors that can be used for prediction of Strongyloides seropositivity among solid organ transplant candidates. Thus, the validity of universal screening was reinforced.
Dr. Jamie Morano, far left, on the panel at “Success Stories in Telehealth.”
Dr. Jamie Morano presented as part of the symposium, “Success Stories in Teleheath,” on “ID Telehealth Best Practices: Veterans Administration.” She presented with Christopher Crnich, MD, and Rima Abdel-Massih, MD, with Moderator John Lynch, MD, also on the podium.
For more information about IDWeek’s 2019 Scientific program, please visit the interactive program page.
Tampa, FL, October 22nd – USF Health’s IDPodcasts Youtube Channel, a production of the Division of Infectious Diseases of the University of South Florida Morsani College of Medicine, announced this week that it has reached its one millionth lifetime view milestone as of October 20, 2019. Although this number is modest in comparison to top 100 YouTube channel rankings with millions of subscribers, IDPodcasts’ subscriber base is #1 among all YouTube Channels belonging to the University of South Florida or its medical affiliates. IDPodcast’s YouTube channel first went online on January 13, 2012, and now has almost 7,000 subscribers.
Although it took more than seven years to reach one million views, according to social media statistics aggregator SocialBlade.com, IDPodcasts’ YouTube channel is projected to double its lifetime views to 2,000,000 by August, 2020, and to achieve its 10,000 subscriber milestone by next summer.
In addition to the latest podcasts obtained from IDPodcast’s website (www.idpodcasts.net), ID Podcast’s YouTube audience can select from more than 250 podcasts taken from IDPodcast’s 12 year history of broadcasting infectious diseases content online. IDPodcasts leverages the talent and teaching skills of the USF Health’s Infectious Diseases (ID) medical faculty and fellows to present compelling ID content for its audience. Select invited national thought leaders in infectious diseases such as Henry Chambers, MD, and Debbie Goff, Pharm.D., have also provided content over the years.
All of IDPodcast’s content is provided free to users, is self-sponsored, and is open access across the online universe. In addition to the YouTube Channel, IDPodcasts offers its content via smartphone and tablet apps, an iTunes Podcast series, and its website. New apps are currently under production for 2019 to bring an enhanced state-of-the-art IDPodcasts listening experience to the latest smartphone devices and tablets.
IDPodcasts was co-founded in 2007 by Dr. Richard L. Oehler, Professor of Medicine at the University of South Florida College of Medicine, and Dr. John T. Sinnott, current Chairman of the Department of Internal Medicine at the Morsani College of Medicine at USF. Dr. Oehler has been its editor-in chief and webmaster since its inception.
An important commentary by IDPodcasts’ editor-in-chief and USF Division of Infectious Diseases Professor, Dr. Richard L. Oehler, is now published in the January 15, 2020 edition of the Infectious Diseases Society of America’s flagship journal, Clinical Infectious Diseases.
The “Viewpoints” article, entitled, “On Measles, Vaccination, Social Media Activism, and How to Win Back Our Role as our Patients’ Best Advocates,” is now available in the print version of the journal.
The article’s focus is about how the recent decline in vaccination rates has led to multiple outbreaks of measles and other vaccine-preventable diseases across the US in 2019. This is surprising, Dr. Oehler notes, “when you consider that less than two decades ago, in 2000, measles was declared eliminated in all 50 states.” Unfortunately, since then, an erosion in public confidence about vaccines and a great resurgence in active measles cases has occurred. At the core of this trend, he writes, is a “perfect storm” of factors:
“The rise of the internet, and the availability of easily accessible but often inaccurate and poorly vetted health information have emboldened patients to make their own medical decisions apart from their provider.” Dr. Oehler explains. “At the same time, the emergence of online social media has permitted like-minded lay people to share online health-related opinions and to engage in healthcare activism. These opinions are magnified in an online echo chamber that has drowned out the voices of a physician community that is often unprepared for communicating in modern ways.”
It is well past time, Dr. Oehler surmises, for the medical community to regain its voice, using smart and sensible tools suitable for the modern era of smartphones and twitter. In his commentary, the author suggests several accessible ways that the medical community can develop its own influencers, bolster and cultivate its own online presence, and leverage social media in positive ways–thus restoring our influential role as our patients’ best advocates.
“Few practicing physicians have heard of Felix Kjellberg, Logan Paul, or Liza Koshy,” Dr. Oehler notes, “but each of these social media celebrities are online superstars known to vast numbers of people worldwide. When either ‘PewDiePie,’ ‘Logan,’ or ‘Liza‘ tweets an idea, promotes a brand, or practices online activism, literally tens of millions of people listen and act. With the exception of a few celebrity media figures (perhaps Bill Nye or Neil Degrasse-Tyson) and physician reporters (Dr. Sanjay Gupta), why can’t the scientific/medial community develop and cultivate more celebrity communicators and online influencers to promote vaccination and other ideas we’re trying to get across to the public? The social media accounts of even major medical organizations can have one-tenth of the followers or less of some accounts run by activist moms from their kitchen counters.”
In addition to his USF teaching responsibilities and editorial responsibilities at IDPodcasts, Dr. Oehler is also a full-time practicing infectious diseases clinician at the James A Haley Veterans Hospital and Moffitt Cancer Center, and the father of two teenagers. “I get plenty of social media exposure [as a parent],” Dr. Oehler asserts.
Tampa, FL, February 5th – USF Health’s IDPodcasts Youtube Channel, a production of the Division of Infectious Diseases of the University of South Florida Morsani College of Medicine, announced today that it has reached its five-thousanth (5000) subscriber milestone as of February 1st, 2019. Although this number is modest in comparison to top 100 YouTube channel rankings with millions of subscribers, IDPodcasts subscriber base is #1 among all YouTube Channels belonging to the University of South Florida or its medical affiliates, exceeding USF Athletics (3,892 subscribers), the USF Channel (3,989 subscribers) Moffitt Cancer Center (4,793 subscribers), Tampa General Hospital (2,300 subscribers) and USF Health (996 subscribers). IDPodcast’s subscriber base also places it ahead of YouTube channels from infectious diseases thought leaders like the National Institute of Allergy and Infectious Diseases [NIAID] (3,038 subscribers) and Medpage today (1,330 subscribers), and within striking distance of popular medically oriented YouTube Channels such as Medscape (16,322 subscribers), NIHvcast (14,596 subscribers)
This year, according to social media statistics aggregator SocialBlade.com, IDPodcasts’ YouTube channel is expected to receive more than 276,000 views from a worldwide audience originating from more than 200 countries. The channel is expected to exceed its next milestone of its one millionth view before the end of 2019.
In addition to the latest podcasts obtained from IDPodcast’s website (www.idpodcasts.net), ID Podcast’s YouTube audience can select from more than 225 podcasts taken from IDPodcast’s 12 year history of broadcasting infectious diseases content online. IDPodcasts leverages the talent and teaching skills of the USF Health’s Infectious Diseases (ID) medical faculty and fellows to present compelling ID content for its audience. Select invited national thought leaders in infectious diseases such as Henry Chambers, MD, and Debbie Goff, Pharm.D., have also provided content over the years.
All of IDPodcast’s content is provided free to users, is self-sponsored, and is open access across the online universe. In addition to the YouTube Channel, IDPodcasts offers its content via smartphone and tablet apps, an iTunes Podcast series, and its website. New apps are currently under production for 2019 to bring an enhanced state-of-the-art IDPodcasts listening experience to the latest smartphone devices and tablets.
IDPodcasts was co-founded in 2007 by Dr. Richard L. Oehler, Professor of Medicine at the University of South Florida College of Medicine, and Dr. John T. Sinnott, current Chairman of the Department of Internal Medicine at the Morsani College of Medicine at USF. Dr. Oehler has been its editor-in chief and webmaster since its inception.
Dr. Ana Velez is an accomplished artist and University of South Florida Associate Professor and Infectious Diseases physician who has practiced at Moffitt Cancer Center among immunocompromised patients since 2007. Her set of paintings, entitled, “Art in Infectious Diseases,” was published on our web site last April to an extremely warm reception from our IDPodcast audience. We received many requests for a follow up to her initial set of works. Dr. Velez has decided to expand her focus to both medical and non-medical classical themes in this collection of works. Enjoy her paintings!
Below is more of her artwork each with an accompanying legend. Please click each picture to link to a larger version.
TITLE:
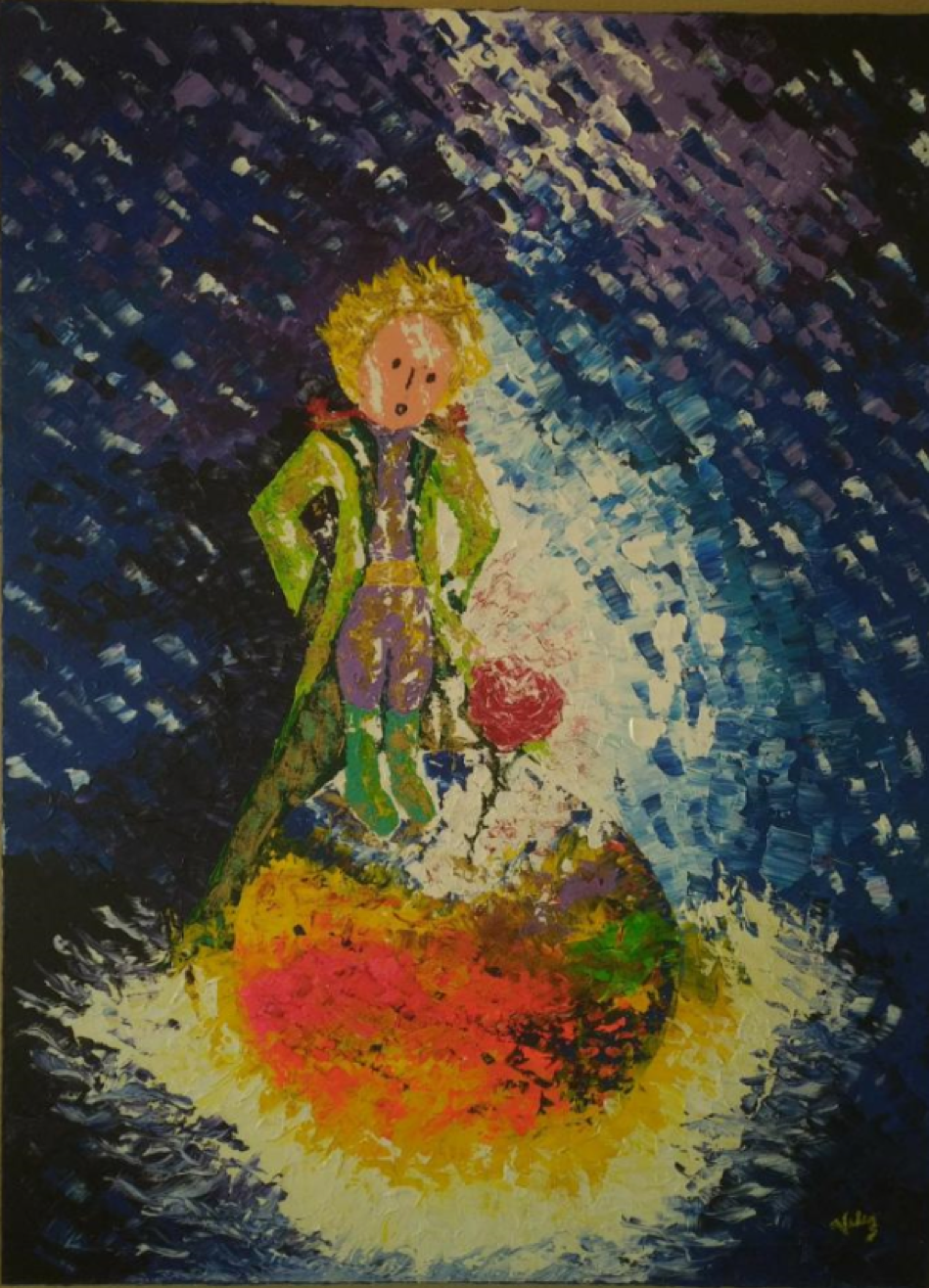
The Little Prince
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
This painting is inspired from the famous novel by Antoine de Saint-Exupéry. It illustrates the life, passion and color that the rose has brought to the little prince’s life.
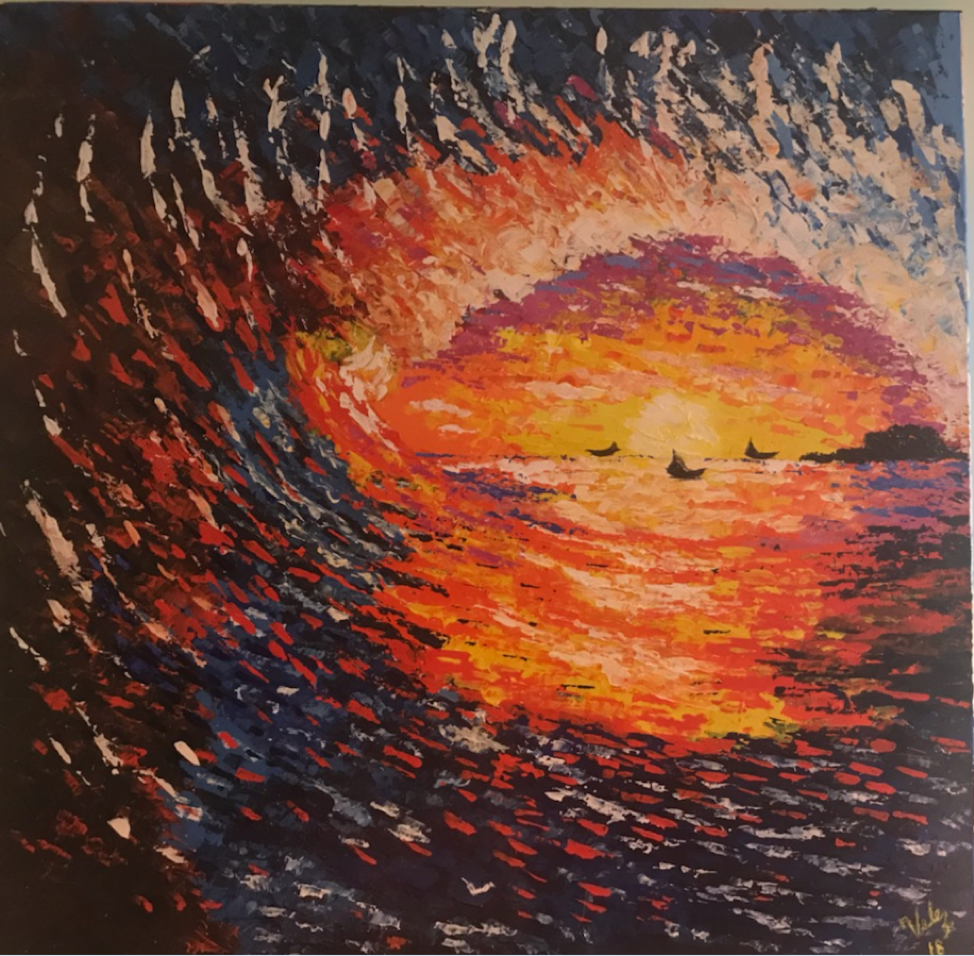
TITLE:
The Wave
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
This painting illustrates the passion, movement, and force of a giant wave during sunset.
From far away it gives a surrealistic view of an eye.
TITLE:
The Dream of the Horse
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
This painting represents the dream of a horse. He is kept in captivity hoping to go back to the wilderness. A colorful sunset of emotions expresses his dream.
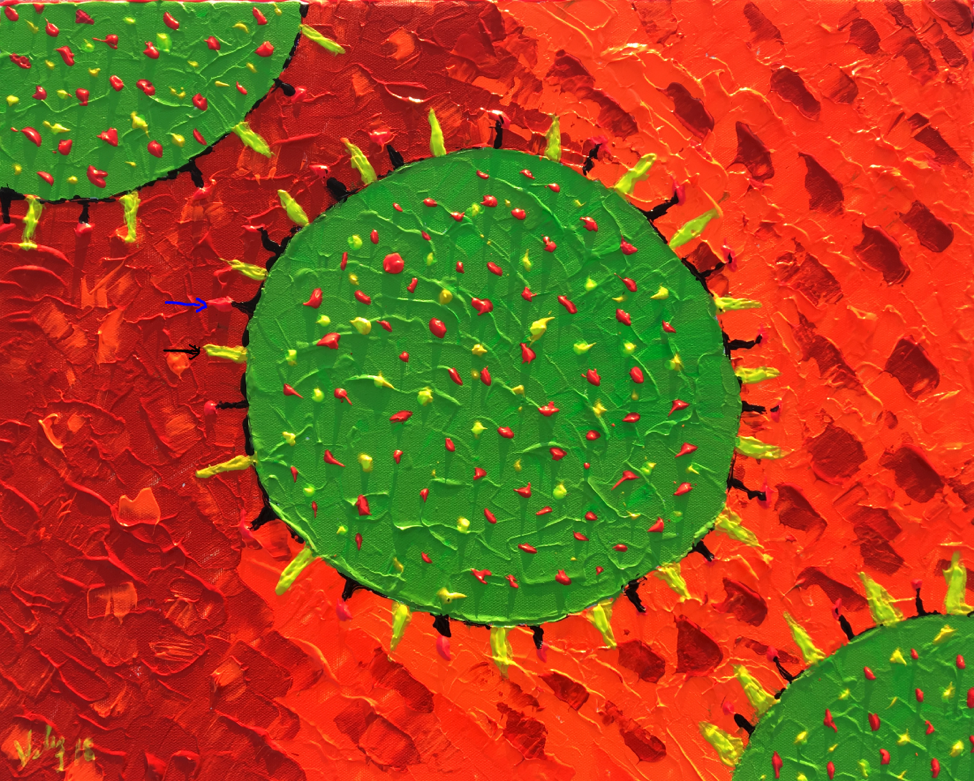
TITLE:
HIV virus
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
HIV virus is an RNA virus that belongs to the lentivirus subfamily of retrovirus. It has a lipid membrane with the trimeric glycoprotein gp 41 (yellow dots) to which the glycoprotein gp 120 ( green dots) is attached.
This painting is an artistic representation of the attachment of the HIV gp120 to the CD4 receptor of the T cell. ( black arrow)
TITLE:
Influenza virus
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
Influenza virus is a spherical RNA enveloped virus that belongs to the Orthomyxoviridae family. The outer layer is a lipid membrane taken from the host cell. Inserted in the membrane are spikes known as hemagglutinin (black arrow)and neuraminidase( blue arrow). These proteins determine the subtype of the influenza virus. Major changes on them are called antigenic shifts and minor changes are called antigenic drifts.
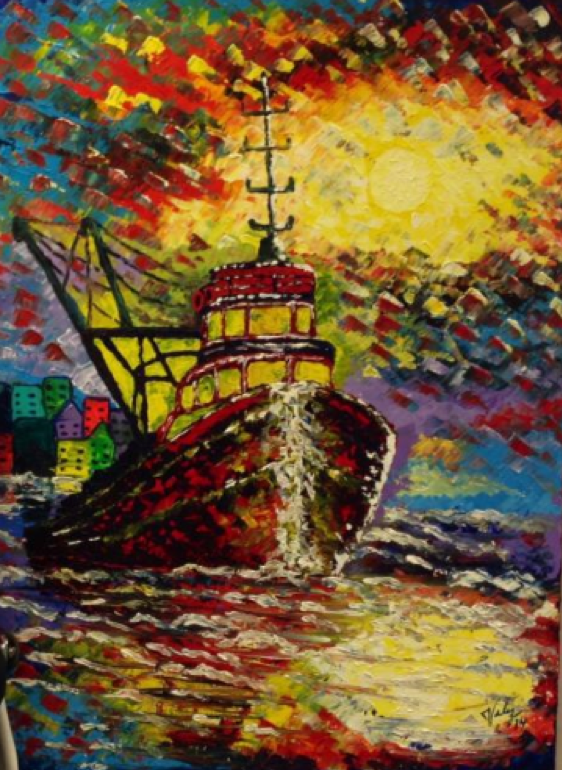
TITLE:
The Captain of the Sea
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
This painting is a gift to my lifelong mentor, Dr. John T. Sinnott, MD, now Chair of Medicine at the University of South Florida Morsani College of Medicine.
The painting represents the challenges that the Chair has to overcome to navigate the turbulent waters of an academic medical program.
Title:
Aedes aegypti
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
Aedes aegypti is a mosquito responsible for the transmission of several viral diseases including dengue, yellow fever, West Nile, chikungunya, eastern equine encephalitis, and Zika.
The mosquito lives in tropical weather, it is more active biting during day time especially early in the morning and before dusk.
It is often recognized by its black and white markings on its body and legs.
TITLE:
ZIKA VIRUS
TECHNIQUE:
Knife painting
Acrylic on canvas
INTERPRETATION:
Zika virus is an RNA virus that belongs to the Flaviviridae family. It is transmitted by the Aedes mosquitoes in tropical and subtropical areas.
Clinical manifestations include low-grade fever, pruritic rash, small joint arthralgia, conjunctivitis, and occasionally infectious complications include Guillain-Barré syndrome, congenital microcephaly and fetal loss among women infected during pregnancy.
The painting above illustrates the outer membrane (yellow arrow) and the dense inner core (white arrow).
The IDPodcasts Team appreciates all the interest we receive on a regular basis for our smartphone and tablet apps. Although we premiered an all new web site in 2018, our app updates have lagged behind. A few months ago, our Android app stopped working due to software compatibility. Our IOS app continues to function, but is sorely in need of new updates.
Fortunately, in 2019, the IDPodcasts platform will welcome new Android and IOS apps! We hope that these new generation apps will include additional functionality that all of our users will enjoy. Specifically, we wish to integrate:
1. Standalone audio podcast compatibility for listening in environments where an audio podcast is appropriate (such as in the car) and where you need your phone for other purposes.
2. Feedback comment capability within the app.
3. More comprehensive indexing.
4. News, blogs, and other features we have added to our web site this year.
While we bring our new apps to completion, for (especially Android) smartphone and tablet users who cannot use our apps, please note that our website is mobile device friendly and should play in any browser. Also, all of our podcast content is still available at our youtube channel at https://www.youtube.com/idpodcasts.
Thank you for supporting our content now for over ten years!
Richard L. Oehler, MD Professor, USF Division of Infections Diseases
Editor, IDPodcasts platforms
Since 2004, I have tried to make IDWeek (formerly known as the “IDSA annual session”) a regular annual event on my professional meeting calendar. Usually held in October, I find this scientific meeting to be a terrific way to connect with long lost colleagues and former fellows, update myself on new science in the form of freshly published abstracts and recently published research, and to refresh my core knowledge in infectious diseases by attending state-of-the-art symposiums and other conference sessions.
This year, IDWeek 18 was held in San Francisco, California from October 2 through October 7. Though the Moscone Center is currently undergoing renovations, making getting around the convention center and Yerba Buena area somewhat more difficult, the pleasant fall San Francisco weather made up for some of the city’s inconveniences.
Conference days at IDWeek can be busy–it is possible to attend as many as 11 hours of scientific sessions each day, and even more if you participate in some of the affiliated (i.e., industry sponsored satellite) meetings. As much as I tried to attend as many sessions as I possibly could, I found my few days at IDWeek to be a balance of scientific meetings, poster sessions, industry exhibits, and connecting (and reconnecting) with friends and colleagues.
As far as the scientific sessions I attended, I needed a few days to reflect on what I had learned before I could put it together in my mind. Now, after being back for a couple of weeks, my chief takeaways from IDWeek are as follows:
Non-tuberculous mycobacterial (NTM) Infections
There was an excellent session on nontuberculous mycobacterial (NTM) infections featuring information on both Mycobacterium avium complex (MAC) and rapid grower mycobacterial (RGM) infections (chiefly Mycobacterium abscessus complex). The presenters made clear the importance of achieving the clinical and microbiologic diagnosis of nontuberculous mycobacterial disease. Traditional diagnostic criteria, of course, emphasize the importance of clinical symptoms, radiographic changes and the exclusion of other diagnoses. The session emphasized the value of a microbiologic diagnosis afforded by either two positive sputum specimens, one BAL specimen and/or appropriate histopathology. The presenters mentioned the need to consider surgical resection of NTM lesions in the presence of geographically discrete disease or when there is failure to respond to medical therapy. Aminoglycoside therapy with amikacin continues to be a critical component of induction therapy in patients who are initiated on an antimycobacterial regimen, but toxicity concerns with aminoglycosides should always be kept in mind. Patients with extensive structural lung disease, resistance to macrolides, and/or persistent smear positivity all are likely to experience poor response to treatment. Similarly, in Mycobacterium abscessus complex disease, the importance of the erm (41) gene as a factor in the treatability of lung disease was emphasized. A significant predictor of progression is low BMI and either bilateral and/or cavitary disease. Some promising new therapies for refractory disease include clofazimine, bedaquiline, and the oxazolidinones; inhaled amikacin and inhaled nitrous oxide therapy may show some promise. Nontheless, NTM lung disease continues to be a frustrating disorder to treat in many severely affected patients.
HIV Disease and Pre-exposure Prophylaxis (PREP)
I was fascinated by a discussion regarding implantable devices useful in preexposure prophylaxis (PREP) for HIV infection. Such devices would be analogous to the Nexplanon contraceptive implant, which provides as much as 3 years of continuous pregnancy prevention. The implants would need to contain extremely potent long-lasting antiretrovirals given their compact size and anticipated life expectancy.
In other HIV news, the recent New England Journal study utilizing Ibalizumab (N Engl J Med 2018; 379:645-654.) in persons with multidrug-resistant HIV was discussed. In this phase 3 trial, 40 heavily treatment experienced patients with multi class antiretroviral resistance were included in the study. After a seven-day control period, a 2 g loading dose was given and functional monotherapy was observed for 7 days. The patients were then started on a regimen optimized to include ≥ 1 fully active agent. Eighty-three percent (83%) of the patients who completed the study achieved the primary endpoint ≥ 0.5 log drop in their viral load after the loading dose (statistically significant). About 43% at week 24-5 had undetectable viral loads. Other advanced therapies discussed during this HIV symposium included a phase 3 trial utilizing fostemsavir, a GP120 blocking agent that inhibits HIV attachment to CD4, PRO 140, a monoclonal antibody against CCR5, and Doravirine, a next generation NNRTI for treating HIV-1 infection. Doravirine has demonstrated non-inferiority to Ritonavir-boosted Darunavir and non-inferior efficacy to Atripla (week 48) in twin phase 3 clinical trials.
Staphylococcus aureus infections
In a symposium on the optimal management of Staphylococcus aureus infections, the authors attempted to answer several pressing questions regarding disease management. Regarding the optimal agent for invasive MSSA infections, the authors presented evidence suggesting that cefazolin therapy is probably better than nafcillin (McDaniel. CID 2017 Jul 1;65(1):100-106.) , but that some caution should be exercised with infective endocarditis and other deep-seated infections. In addition, some MSSA strains exhibited what was called the Cefazolin inoculum effect (CzIE), which resulted in the development of high MICs (≥ 16 ug/ml when the strains were incubated with high colony concentrations of MSSA (~107 CFU/mL) versus standard colony counts (~105 CFU/mL). The authors concluded that the clinical significance of CzIE is unclear. For treatment of MRSA bacteremia, the speakers presented data suggesting that for MRSA bacteremia with a vancomycin MIC ≥ 1.5, an early switch to daptomycin was associated with better outcomes. Furthermore, in a multicenter retrospective cohort in cases of MRSA bacteremia with a vancomycin MIC > 1, failure rates were similar and there was less kidney injury in the daptomycin group. Regarding whether combination therapy is useful in the treatment of Staphylococcus aureus bacteremia, data was presented (Thwaites, et. al. Lancet 2018;391:668-78.) suggesting that there was no 30 or 90 day mortality benefit in the addition of a beta lactam plus a second agent (typically, rifampicin, a fluoroquinolone, an aminoglycoside or fosfomycin) except for adding rifampin when there is prosthetic material. When considering oral stepdown therapy for the treatment of endocarditis, there have long been questions about how effective partial or fully oral regimens are for the treatment of Staphylococcus aureus endocardits. This is particularly true in cases where a prolonged course of IV therapy is not possible or carries significant safety risks. The recent NEJM POET study (Iverson. NEJM 2018) looked at 400 patients with left-sided gram-positive endocarditis and compared outcomes in those who received at least 10 days IV therapy and then were either switched to oral therapy or continued on intravenous agents. The most common oral regimens were either dicloxacillin plus rifampin or amoxicillin plus rifampin. The findings applied to MSSA only and in patients with no extracardiac complications. The study showed that in patients with endocarditis on the left side of the heart who were in stable condition, changing to oral antibiotic treatment was noninferior to continuing intravenous antibiotic treatment. However, the same results do not apply to MRSA cases. Lastly, regarding salvage options for highly resistant Staphylococcus aureus, data was presented suggesting some utility for the combination of daptomycin and ceftaroline based upon a recent multicenter observational study (Zasowski, et. al. AAC 2017).
Opioid Use Disorder
Many clinicians attended a session on the importance that infectious diseases providers can play in the management of opioid use disorder when we intervene for infectious complications of their substance use. This discussion included information on so-called “supervised safer injection facilities” (SIS) where substance users can safely inject IV drugs under the nonjudgmental supervision of healthcare providers. Nearly 100 of these SIS facilities are in existence in Canada, Europe and Australia, but so far, are only apparently being considered or debated in the United States. The symposium presenters asserted that literature suggests that such supervised facilities reduce infectious diseases transmission, improve overdose morbidity and mortality, increase access to healthcare, do not increase crime or public disorder, and are cost effective. It remains to be seen if such facilities gain a foothold in U.S. communities (such as San Francisco) with significant IVDA populations.
Klebsiella pneumoniae, CRE, and HvKP
In a symposium regarding the “Big Beasts” of infectious diseases, two “Big Beasts” of Klebsiella pneumoniae were discussed, including hyper virulent Klebsiella pneumoniae (HvKP) and, Carbapenemase-producing Klebsiella pneumoniae (CRKP). First described in Taiwan in the 1980s as a cause of pyogenic liver abscess, HvKP is an emerging cause of community-acquired infections in immunocompetent hosts. This strain of Klebsiella can produce a variety of systemic manifestations, including necrotizing fasciitis, osteomyelitis, and meningitis. Fortunately, HvKP appears to be less likely to demonstrate multidrug resistance in comparison to “classic” Klebsiella pneumoniae. CRKP continues to become a more significant cause of hospital-acquired infections, most recently associated with duodenoscopes. Emerging treatments for carbapenemase resistant Enterobacteriaceae (CRE) include cefazidime-avibactam, plazomycin (a new novel aminoglycoside), meropenem-vaborbactam, imipenem-relabactam, aztreonam-avibactam, and cefiderocol. There is concern that these twin strains may share resistance factors via plasmid-related convergence, leading to hyper virulent MDR Klebsiella pneumoniae.
Febrile Neutropenia
The management of febrile neutropenia was discussed in a separate symposium with regard to bloodstream infections, particularly those with ESBL positive Enterobacteraceae. The recent MERINO trial (Harris, et. al. JAMA. 2018;320(10):984-94.) involved 26 hospitals worldwide and looked at 30 day mortality when Escherichia coli and Klebsiella pneumoniae ESBL positive bloodstream infections were treated with piperacillin-tazobactam versus meropenem. This study found that the 30-day mortality was significantly higher (12.3%) in the Piperacillin-Tazobactam group than in the meropenem (3.7%) group. Conversely, the mortality associated with carbapenemase-resistant gram-negative bacteremia was significantly greater, suggesting that carbapenem use should still be restricted to reduce the emergence of carbapenemase-resistant Pseudomonas, Acinetobacter and Enterobacteraceae. A study by the European conference on infections including leukemia published by Mikulska in the Journal of infection (Mikulska, et. al. J Infect 2018;76(1):20-37.) was also discussed. This review showed no reduction in mortality through the common use of fluoroquinolone prophylaxis in prolonged neutropenic patients (> 7 days), although rates of bloodstream infection and fever episodes were decreased. The review suggested that fluoroquinolone prophylaxis should be utilized in high-risk patients only and be dependent upon local epidemiology and practice.
Fun and Games
Unfortunately, IDWeek is far too large a meeting for the totality of its expansive and compelling scientific program to be described here. For me, a highlight was clearly the 3rd annual ID Bug Bowl. This is the annual infectious diseases quiz competition that caps off the meeting, usually on the evening prior to the closing plenary. Even though we here at IDPodcasts still lay first claim to the term “Bug Bowl,” (Our “Bug Bowl: Bacteriology edition” podcast appeared online in 2015 the year before the first IDWeek session was inaugurated in 2016), we still try to attend every year to take in some of the excitement and “infectious” enthusiasm (pun intended) conveyed by the medical students, residents, and infectious diseases fellows from 3 or 4 different institutions who are its participants. This year, Wake Forest University and University of Kansas Medical Center battled local San Francisco institutions UCSF and Stanford University for more than an hour in a Jeopardy-style format. After “FINAL IDBugBowl,” which all participants wagered on their answer to the question, “Oculomasticatory mylorythmia is pathognomonic for this infectious disease,” Stanford University was declared the winner. Congratulations to them and all the participants!
If you know which infectious disease is associated with “Oculomasticatory mylorythmia,” please answer in the comment section of this blog. Next year’s IDWeek will be held in Washington DC on October 2-6, 2019.
As I often do, I recently spent a few moments on a Friday morning reviewing the CDCs “Current Outbreak List” page. This resource is a single page clearinghouse for recent United States and international outbreaks reported on by the Centers for Disease Control and Prevention. On the day I reviewed the page, recent Salmonella-based outbreaks in breakfast cereal, pre-cut melon, live poultry and backyard flocks and pet guinea pigs were mentioned. Other Salmonella-related outbreaks occurring in 2018 included dried coconut, chicken salad, Kratom, raw sprouts, cucumbers, and papayas.
The predominance of Salmonella among food-borne pathogens is not surprising, as non-typhoidal Salmonellae in the US is one of the leading causes of foodborne disease. It is also a major cause of worldwide diarrhea. The high prevalence of non-typhoidal salmonellosis in the food supply has been primarily associated with agricultural reservoirs, most commonly with poultry and chicken eggs. In recent years, outbreaks associated with raw produce have increased in prevalence, perhaps related to contamination of the food chain resulting from run off from animal agricultural lots, or the secondary cross-contamination of produce during harvesting, processing, or food preparation. Yet this is not a new phenomenon. Foodborne outbreaks have been an issue in the U.S. food industry for decades.
In the course of researching this topic, I came across a media report entitled, “Expert: Technology could help make food safer.” The article was an interview of Dr. Dennis Maki, a well-known professor in epidemiology at the University of Wisconsin School of Medicine and Public Health. Dr. Maki noted that the era of feeding 300 million plus people through the use of small farms and simple agricultural techniques has long since passed.
Dr. Maki said,
“it’s important to realize there are 300 million people in the US. The only way you are going to feed 300 million people is by industrial techniques. The common complaint or the plea is, ‘lets return back to 1945, let’s have small farms, let’s not have industrial farming and industrialized production of food on a huge scale. Then we wouldn’t have the problems that we have now.” But such an approach would not result in the ability of our agricultural industry to feed a 21st Century population, he asserted.
Dr. Maki emphasized several approaches for the consumer to reduce their likelihood of acquiring foodborne illness. (1) Buy food from reputable sellers. Most large grocery chains are highly reputable, or they would not be in business. (2) Wash fruits and vegetables thoroughly as this will greatly reduce, though not completely eliminate contamination. (3) Cook meats properly and to the recommended temperature.
The article featuring Dr. Maki, though very relevant today, was not from 2018, but 2007. And over the last decade, seemingly very few manufacturing components of the agricultural industry appear to have changed. However, the grocery marketplace continues to emphasize foods that are more “natural,’ ‘organic,’ or preservative-free. Similarly, upscale grocery chains promote food products that are marketed as being less associated with the food-industrial complex (grain fed beef, cage-free eggs, organic sprouts, etc.). At the same time, the public’s insatiable demand for all-season produce results a food distribution system that needs to be worldwide. (i.e., grapes from Chile, avocados from Mexico, pineapples from Thailand, oranges from Brazil, figs from Turkey, etc.)
So the original question in the 2007 article still applies today: “Can technology reduce infection in our food?” One of the most fascinating and progressive areas where technology is pushing the envelope is in the meat industry. American consumers eat 26 billion pounds of beef a year. A single cow is said to consume up to 11,000 gallons of water annually. The fast food chain McDonald’s cells 75 hamburgers every second. As a result, the cultivation of meat products requires a huge worldwide industry that is estimated to be responsible for 15-20% of all greenhouse gas emissions. Furthermore, the production of the millions of poultry, pork and beef livestock animals places considerable demands on agricultural areas to contain and manage the tremendous quantities of animal waste and other industrial byproducts of meat processing, much of which is at risk for contamination of the environment and at various points in the food chain.
As a result, several Silicon Valley technology start ups have for several years now been working on different lab-based techniques for the production of meat. The concept in itself is deceptively elementary: What if the production of meat could be made as simple as growing yeast in a vat? If we could turn the philosophy of, “kill it and grill it” to “fill it and then distill it.” If we could culture meat in a lab and then grow it utilizing industrial techniques similar to beer production, this would eliminate a large proportion of the land use, water consumption, greenhouse gas admissions, and production of animal byproducts that result in the runoff of enteric pathogens such as Salmonella and the contamination of the environment and of our food.
Just, a Silicon Valley company, is perhaps the leader in attempts to bring the first “clean meat” products to market. Their process involves the development of a large-scale cell culture process for cultivating sustainable meat cells into high-grade meat and seafood with a production process that promises to be over 10 times more efficient then the world’s largest slaughter houses. They claim their process uses unmodified cells which naturally occur in livestock animals and can be grown antibiotic free. Because the process does not involve slaughtering live animals, they claim their manufacturing chain will have a significantly lower risk of foodborne illness (and be much less negatively impactful on the animals in general). Other lab-based meat companies looking to develop similar technologies include Memphis Meats and Future Meat Technologies.
Such food technology elicits a wide variety of reactions from the public, ranging from those who say, “I would never eat that,” to individuals who claim that “cultured meat is not natural,” to the more adventurous who boast, “I’ll eat it if it tastes good and is safe.” But the history of food in the U.S. suggests that similar battles have been waged in the past, from the adoption of margarine as a butter substitute in the late 19th Century to the rise of nut-based milk products (e.g., soy milk, almond milk, etc) in the last 15 years, with the new products ultimately finding acceptance if they are felt to be economical, healthier, and no less palatable than their traditional counterparts. But with the production of meat and seafood estimated to double to 1.2 trillion pounds by 2050, given a finite land supply and limited environimental resources, current industrialized processes for meat and food production are unsustainable, and new techniques are clearly needed.
The development of cultured meat products has led to an industry debate, led mainly by traditional agricultural industry firms and trade associations, on what constitutes the terms “meat” and “beef” at all. The FDA will hold public hearings on this topic this summer.
As consumers, all of us can play a role in ensuring the safety of the U.S. food system in the products we consume, the choices we make, the food preparation techniques we use, and in the ways we maintain awareness of what is going on with our food supply.
Please note that the opinions expressed in this blog post are my own and do not necessarily reflect the views of IDPodcasts, the Division of Infectious Diseases, USF Health, or the University of South Florida.
There’s an expression I’ve often seen online — “what a difference a decade makes.” And it resonates across many epochs of our recent history. Historians can look at the transition our country made in the 1960’s, for instance, and see the United States emerging from the consumer-based post-war era of the late 1950s to the turbulent and transformative year of 1969 as indicative of how much things can change over 10 years.
As I reflect upon IDPodcast’s ten-year milestone, recently celebrated in 2017, I think about the many ways medicine, education and society have changed since 2007, when I first sat down with our Chief of Infectious Diseases and IDPodcasts’ co-founder, Dr. John T Sinnott, to look at ways that USF’s Division of Infectious Diseases could broaden its outreach and share its teaching excellence beyond the small community of medical students, residents, and clinical faculty that had been attending our conferences for many years. I credit Dr. Sinnott with the original idea of broadening our educational footprint, when I recall him saying, “why don’t you take these lectures, record them, and place them online on a website.”
A light went on in my head. A website for infectious diseases podcasts, “IDPodcasts,” I thought. “Wait a minute. If we recorded these lectures, then maybe I and others can listen to them on an iPod.” I immediately started thinking of how I could set up and design a website and get us online.
It’s easy to forget: In early 2007, most online content was limited to desktop computers or laptops. Portable content was available only through mobile MP3 players such as the iPod. (Thus, the name, “POD-casts.”) Although the iPhone was first announced in January, 2007, it was not released to consumers until July of that year. The first iPhone had no installable apps, sluggish 2G (EDGE) connectivity, and a relatively tiny low resolution screen. Tablets did not exist at that time.
Online streaming was in its infancy in 2007. YouTube had just been acquired by Google the year before, and was relatively not well known by online users.
YouTube in 2006. (Source, Wayback Machine)
Other educational online streaming sites were also in figurative diapers. Khan academy was founded in October, 2006, but did not offer regular online content until 2008. Most educational medical content was distributed via VHS Cassette, CD-Rom or DVD.
After IDPodcasts established itself as the very first infectious diseases online podcast site, we started looking at other ways we could share content online. Given the popularity of iPods during that time, we inaugurated IDPodcasts’ iTunes Podcast Channel in 2008.
While our website was attending to establish a foothold online, another revolution was rapidly advancing in the mobile universe—smartphones. The first mobile online applications were being introduced with the next generation iPhone, and our quest to capture medical users of smart phone devices became our next initiative. In 2009, we partnered with Absolute Mobile Solutions in Tampa, Florida to create our first IDPodcasts app. The IDPodcasts mobile viewer was the first streaming iPhone app at the University of South Florida and the entire state of Florida University system.
As mobile online devices became more popular, device manufacturers soon began to innovate and look for more ways that mobile devices could replace traditional desktop or laptop computers. In 2010, the iPad was born, and IDPodcasts introduced the first iPad app created at the University of South Florida, and then introduced a sister app for android mobile devices.
In 2011, the website introduced social media integration into its main page, permitting users to be notified through their Facebook or Twitter pages of new online content. To capture users of the increasingly popular streaming site, YouTube, in 2012, we inaugurated the IDPodcasts YouTube channel, which has gone on to become one of our most successful online sites with thousands of views.
Our latest generation smartphone and tablet apps premiered in 2016, incorporating many new features such as favorite and playlists, Apple watch controls, enhanced search features, and social media integration.
We commemorated our tenth anniversary in 2017 with the “IDPodcaster awards,” celebrating the best of our podcast presentations over our history. And as we began our second ten years in 2018, IDPodcasts premiered its most significant upgrade yet: A brand new website designed for maximum usability, speed, and performance across any desktop, portable, or handheld device. And we look forward to even more refinements and enhancements moving forward. This includes our new blog feature, which recently has highlighted the artistic and literary talents of our faculty and invited contributers.
Throughout the last ten-plus years, IDPodcasts has continued to publish high-quality, well produced, and educationally innovative content at no cost to our listeners. We accept no commercial sponsorship, relying on university and small contributor support. Our biggest reward is the feedback we get from our listeners, including clinicians and lay people from more than 160 countries around the world. Our goal, as our new slogan suggests, is to simply “make infectious disease learning contagious.”
IDPodcasts owes a huge debt of gratitude to its cofounder and Chief of the Department of Internal Medicine, Dr. John T. Sinnott, as well as the Division of Infectious Diseases Director, Dr. Douglas Holt, for their unwavering support of this decade-long educational initiative. And ID podcasts is especially indebted most of all to its more than 60 faculty contributers who have shared their teaching excellence with a worldwide audience over more than 10 years, as well as its loyal online audience.